

Introduction
High risk (HR) multiple myeloma (MM) constitutes approximately 25 % of newly diagnosed patients and is a subgroup of MM patients that is variably defined. Patients with 17p deletion are considered HR and their optimal treatment approach has not been determined. Various strategies have been suggested to improve outcomes in MM patients harboring del 17p, including tandem transplants. Recently, the long-term outcomes of the phase 3 EMN02 trial were published with the study group receiving bortezomib, cyclophosphamide and dexamethasone (VCd) induction prior to transplant. There are no data demonstrating that tandem transplant is applicable to the US population using induction containing immunomodulatory agents and bortezomib.
Aim
To report on outcomes of newly diagnosed MM patients with del 17p that underwent autologous stem cell transplantation (ASCT).
Methods
Retrospective study of all consecutive newly diagnosed MM patient with del 17p that underwent ASCT at Mayo Clinic, Rochester, Minnesota. Patients were defined by the Mayo Medical Lab as 17p deleted and included if they met the following criteria: If 50 cells in the bone marrow sample and 10 cells with the deletion were identified (20%) or if the bone marrow sample had between 20-50 total cells and 20% cells with the deletion were identified. We excluded patients that relapsed prior to ASCT (as those patients were excluded in the EMN02 trial), patients that underwent ASCT more than 12 months from the diagnosis and patients that underwent tandem ASCT (defined as two consecutive ASCT within 180 days of each other without relapse in between). Consolidation treatment was defined as treatment given after transplant for up to six 28-day cycles and maintenance was defined as all treatment given after ASCT for more than 6 months. Combined maintenance was defined as maintenance regimens that included two novel agents.
Results
116 patients with MM and 17p deletion underwent ASCT at Mayo Clinic between January 2013 and April 2020. The median age at diagnosis was 62 (IQR 57-68, range 34-76) years. Forty-five (39%) patients were over 65 years. Nine patients (8%) had triple-hit MM and 34 (29%) had double-hit MM. Median follow-up of the survivors was 33 months (IQR 21-54). Consolidation therapy was given to 36 patients (31%) and maintenance was given to 91 patients (78%). Seven patients relapsed before day 100.
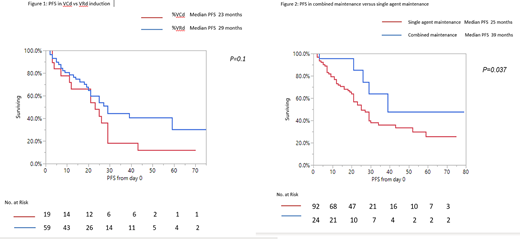
There was no difference in the OS (P=0.72) or PFS (P=0.1) between patients that received VRd (bortezomib, lenalidomide and dexamethasone) versus VCd (bortezomib, cyclophosphamide and dexamethasone) induction (Figure 1). When comparing patients that received proteasome inhibitors (PIs)+ immunomodulatory agents (IMiDs) as induction to patients that received VCd induction, PFS was longer for patients that received the PIs + IMiDs (HR 0.53 P=0.04, 95% CI=0.3-0.98) (Figure 2), however there was no OS difference (P=0.61).
Maintenance therapy was given to 94 patients (81%). There was no OS (P=0.34) or PFS (P=0.36) difference between IMiD based and PI based maintenance, but there was a PFS advantage to patients that received two drug maintenance (HR= 0.41, P=0.037, 95% CI 0.14-0.95) (Figure 2).
The median OS and PFS of the entire cohort were not reached and 29 months, respectively.
Conclusions
The outcomes of our patients were similar to that of the single arm ASCT in the EMN02 trial, and no difference in outcomes were found between patients that received VRd and VCd induction, suggesting that tandem transplants should be considered for 17p deleted MM patients. Dual novel agent maintenance therapy is important in improving outcome.
Kapoor:Celgene: Honoraria; GlaxoSmithKline: Research Funding; Sanofi: Consultancy, Research Funding; Amgen: Research Funding; Cellectar: Consultancy; Takeda: Honoraria, Research Funding; Janssen: Research Funding. Kumar:Takeda: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Dr. Reddy's Laboratories: Honoraria; AbbVie: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Celgene/BMS: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Sanofi: Research Funding; Cellectar: Other; Genecentrix: Consultancy; Tenebio: Other, Research Funding; Adaptive Biotechnologies: Consultancy; Janssen Oncology: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Genentech/Roche: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Oncopeptides: Consultancy, Other: Independent Review Committee; IRC member; Kite Pharma: Consultancy, Research Funding; Merck: Consultancy, Research Funding; Amgen: Consultancy, Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments, Research Funding; Novartis: Research Funding; Carsgen: Other, Research Funding; Karyopharm: Consultancy; BMS: Consultancy, Research Funding; MedImmune: Research Funding. Dispenzieri:Pfizer: Research Funding; Takeda: Research Funding; Janssen: Research Funding; Alnylam: Research Funding; Intellia: Research Funding; Celgene: Research Funding. Dingli:Alexion: Consultancy; Sanofi-Genzyme: Consultancy; Bristol Myers Squibb: Research Funding; Janssen: Consultancy; Millenium: Consultancy; Karyopharm Therapeutics: Research Funding; Rigel: Consultancy; Apellis: Consultancy. Gertz:DAVA oncology: Speakers Bureau; Proclara: Other; Abbvie: Other; Physicians Education Resource: Other: personal fee; Medscape: Other: personal fee, Speakers Bureau; Appellis: Other: personal fee; Research to Practice: Other; Ionis/Akcea: Other: personal fee; Celgene: Other; Teva: Speakers Bureau; Johnson and Johnson: Speakers Bureau; Annexon: Other: personal fee; Alnylam: Other: personal fee; Prothena: Other: personal fee; Janssen: Other: personal fee; Spectrum: Other: personal fee, Research Funding; Aurora Bio: Other; Springer Publishing: Patents & Royalties; Sanofi: Other; Amgen: Other: personal fee.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal